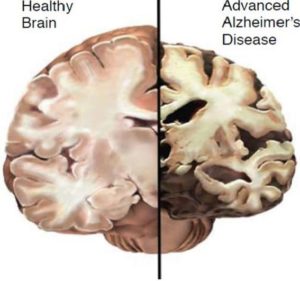
ALZHEIMER’S DISEASE IS REVERSIBLE – MEMORY CAN BE RESTORED
A Summary of the New Path for Healing
NIH National Institute of Aging – the conventional medical perspective
- “Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks.”
- “Alzheimer’s disease is currently ranked as the sixth leading cause of death in the United States, but recent estimates indicate that the disorder may rank third, just behind heart disease and cancer, as a cause of death for older people.”
 Alzheimer’s disease: a sad story until now
Alzheimer’s disease: a sad story until now
- PATIENTS often do not seek medical care because they have been told there is nothing that can be done, and they fear loss of driver’s license, the stigma of a diagnosis, inability to obtain long-term care, and ultimately nursing home placement. Thus they often present very late in the process
- PRIMARY CARE PROVIDERS often do not refer, since they realize that there is no truly effective therapy. Therefore, they typically simply start donepezil (Aricept), often without a firm diagnosis.
- SPECIALISTS often put the patients through hours of neuropsychological testing, expensive imaging, lumbar punctures, and then have little or nothing to offer therapeutically.
A New Story: Reversal of cognitive decline using integrative medicine
Dale E. Bredesen AGING, September 2014, Vol 6 N 9
- Abstract: This report describes a novel, comprehensive, and personalized therapeutic program that is based on the underlying pathogenesis of Alzheimer’s disease, and which involves multiple modalities designed to achieve metabolic enhancement for neurodegeneration (MEND)
- The first 10 patients who have utilized this program include patients with memory loss associated with Alzheimer’s disease (AD), amnestic mild cognitive impairment (aMCI), or subjective cognitive impairment (SCI).
- Nine of the 10 displayed subjective or objective improvement in cognition beginning within 3-6 months, with the one failure being a patient with very late stage AD.
Alzheimer’s disease statistics www.alz.org
- 3 million (1 in 9 over age 65) have AD (200,000 under age 65)
- By 2050 that number will nearly triple.
- 1 in 3 by age 80 (1 in 2 by age 85)
Facts about Alzheimer’s disease
- Alzheimer’s disease is the most common type of dementia.
- It happens when plaques containing beta amyloid form in the brain.
- As symptoms worsen, it becomes harder for people to remember recent events, to reason, and to recognize people they know.
- Eventually, a person with Alzheimer’s is likely to need full-time assistance.
Big Pharma: searching for a drug
- in the past decade alone, hundreds of clinical trials have been conducted for AD, at an aggregate cost of billions of dollars, without success.
- there is not a single therapeutic that exerts anything beyond a marginal, unsustained symptomatic effect, with little or no effect on disease progression.
 Symptoms: The cognitive decline must be seen in at least two of the five symptom areas listed below:
Symptoms: The cognitive decline must be seen in at least two of the five symptom areas listed below:
- Reduced ability to take in and remember new information, for example
- repetitive questions or conversations
- getting lost on a familiar route
- Impairments to reasoning, complex tasking, and exercising judgment, for example:
- poor understanding of safety risks
- inability to manage finances
- Impaired visuospatial abilities that are not, for example, due to eye sight problems. These could be:
- inability to recognize faces or common objects or to find objects in direct view
- inability to use simple tools, for example, to orient clothing to the body
- Impaired speaking, reading and writing, for example:
- difficulty thinking of common words while speaking, hesitations
- speech, spelling, and writing errors
- Changes in personality and behavior, for example:
- out-of-character mood changes, including agitation, apathy, social withdrawal or a lack of interest, motivation, or initiative
- loss of empathy
 Caution! These 10 Drugs Can Cause Memory Loss (AARP, Dr. Armon B. Neel, Jr)
Caution! These 10 Drugs Can Cause Memory Loss (AARP, Dr. Armon B. Neel, Jr)
- Antianxiety drugs
- Cholesterol drugs
- Antiseizure drugs
- Antidepressant drugs
- Narcotic painkillers
- Parkinson’s drugs
- Hypertension drugs
- Sleeping aids
- Incontinence drugs
- Antihistamines
Alzheimer’s disease: insights from epidemiology.
McDowell I. Aging (Milano) 2001 Jun;13(3):143-62
- Women generally appear at higher risk than men, as do people with lower levels of education
- Depression is probably a precursor
- Head injury is an established risk factor and may interact with the apolipoprotein E gene;
- Several occupational exposures appear hazardous, and exposure to aluminum in the water supply confers excess risk. Risk is nearly double.
- Hypertension and other vascular symptoms appear to predispose to AD, which is now seen as closer to vascular dementia than was previously believed.
- The use of non-steroidal anti-inflammatory drugs to treat arthritis is associated with a reduced risk of AD
- Estrogen use by post- menopausal women is associated with reduced risk
- Physical activity appears beneficial,
- diet with high levels of vitamins B6, B12, and folate is protective
- Red wine in moderate quantities appears protective (Resveratrol?).
Alzheimer’s disease – Diagnoseable 9 years before symptoms
Amyloid Plaques
- The beta-amyloid protein involved in Alzheimer’s comes in several different molecular forms that collect between neurons.
- abnormal levels of this naturally occurring protein clump together to form plaques that disrupt cell function.
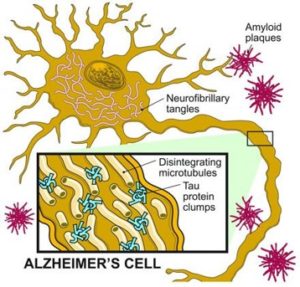 Neurofibrillary Tangles
Neurofibrillary Tangles
- abnormal accumulations of a protein called tau that collect inside
- abnormal chemical changes cause tau to detach from microtubules and stick to other tau molecules, forming threads that eventually join to form tangles inside neurons.
- These tangles block the neuron’s transport system, which harms the synaptic communication between neurons.
Fungal infection in patients with Alzheimer’s disease
Alonso R, et al J Alzheimer’s Dis. 2014;41(1):301-11
- This disease is characterized by the presence in the brain of amyloid plaques and neurofibrillary tangles that provoke neuronal cell death, vascular dysfunction, and inflammatory processes.
- In the present work, we have analyzed the existence of fungal infection in Alzheimer’s disease patients.
- A proteomic analysis provides compelling evidence for the existence of fungal proteins in brain samples from Alzheimer’s disease patients.
- Furthermore, PCR analysis reveals a variety of fungal species in these samples, dependent on the patient and the tissue tested.
- To our knowledge these findings represent the first evidence that fungal infection is detectable in brain samples from Alzheimer’s disease patients
Dr William Shaw – Great Plains Labortory
- A number of tests have been carried out in blood serum, including the detection of antibodies against several yeast species and fungal proteins
- Results indicate that there is disseminated fungal infection in the majority of AD patients tested.
 Why Plaque Attacks: A bold theory—that the brain-tangling proteins of Alzheimer’s disease may form to fight infection
Why Plaque Attacks: A bold theory—that the brain-tangling proteins of Alzheimer’s disease may form to fight infection
- Researchers took autopsied brain tissue from a region of the brain that was ravaged by Alzheimer’s
- the homogenized tissue was lethal to microbes 100 times more potent than penicillin.
The fetal basis of amyloidogenesis: exposure to lead and latent overexpression of amyloid precursor protein and beta-amyloid in the aging brain.
Basha, MR, The Journal of Neuroscience,January 26, 2005, 25(4):823-829
- Rats exposed neonatally to low levels of lead have increased amyloid deposits in their brains in old age, implicating early lead exposure in the causation of Alzheimer’s disease.
- The exposure permanently alters the behavior of the APP gene, which produces the amyloid peptide.
- Exposure in old age to the same lead level, however, did not produce the effect.
- These results suggest Alzheimer’s may be one of an increasing number of adult diseases caused by early child exposure to heavy metals.
 Does inorganic mercury play a role in Alzheimer’s disease? A systematic review and an integrated molecular mechanism.
Does inorganic mercury play a role in Alzheimer’s disease? A systematic review and an integrated molecular mechanism.
J Alzheimer’s Dis. 2010;22(2):357-74. Mutter J
- 32 studies out of 40 testing memory in individuals exposed to inorganic mercury, found significant memory deficits.
- Autopsy studies found increased mercury levels in brain tissues of AD patients.
- In vitro models showed that inorganic mercury reproduces all pathological changes seen in AD, and in animals inorganic mercury produced changes that are similar to those seen in AD.
Would decreased aluminum ingestion reduce the incidence of Alzheimer’s disease?
McLachlan DR, Canadian Med Assoc j1991 Oct 1;145(7):793-804
- evidence that implicates aluminum as a toxic environmental factor
- Laboratory studies of the effects of intracerebral aluminum on the cognitive and memory performance of animals,
- Slowing of the progress of the disease with the use of an agent that removes aluminum from the body
Aluminum hydroxide injections lead to motor deficits and motor neuron degeneration
Shaw, CA et al, J Inorg Biochem. 2009 November ; 103(11): 1555
- Aluminum-treated mice showed significantly increased apoptosis of motor neurons and increases in reactive astrocytes and microglial proliferation within the spinal cord and cortex.
- Found aluminum in the cytoplasm of motor neurons with some neurons also testing positive for the presence of hyper- phosphorylated tau protein, a pathological hallmark of various neurological diseases, including Alzheimer’s disease and frontotemporal dementia.
- A second series of experiments was conducted on mice injected with six doses of aluminum hydroxide. Behavioural analyses in these mice revealed significant impairments in a number of motor functions as well as diminished spatial memory capacity.
 Mechanisms of Mycotoxin-Induced Neurotoxicity through Oxidative Stress-Associated Pathways
Mechanisms of Mycotoxin-Induced Neurotoxicity through Oxidative Stress-Associated Pathways
Kunio Doi. Et al, Int J Mol Sci. 2011; 12(8): 5213–5237, 2011 Aug 15.
- Among many mycotoxins, T-2 toxin, trichothecenes, fumonisin B1 (FB1) and ochratochin A are known to have the potential to induce neurotoxicity in rodent models.
- T-2 toxin induces neuronal cell apoptosis in the fetal and adult brain.
- Trichothecenes bring about neuronal cell apoptosis and inflammation
- FB1 induces neuronal degeneration in the cerebral cortex
- Ochratoxin causes acute depletion of striatal dopamine and its metabolites, with neuronal cell apoptosis in the substantia nigra, striatum and hippocampus.
Adult hippocampal neural stem/progenitor cells in vitro are vulnerable to the mycotoxin ochratoxin-A.
Sava V, et al, Toxicol Sciences. 2007 Jul;98(1):187-97
- The common mycotoxin ochratoxin-A accumulates in brain, causes oxidative stress, and elicits a DNA repair response that varies across brain regions and neuronal populations.
- OTA exposure may contribute to impaired hippocampal neurogenesis in vivo, resulting in:
- Depression
- memory deficits
Inhalational Alzheimer’s disease: an unrecognized – and treatable – epidemic.
Bredesen, Aging (Albany NY). 2016 Feb;8(2):304-13
- Alzheimer’s disease is the result of exposure to specific toxins, and is most commonly inhalational (IAD), due to mycotoxins.
Alzheimer’s disease – a neurospirochetosis. Analysis of the evidence
Miklossy J, J Neuroinflammation. 2011 Aug 4;8:90..
- When neutral techniques recognizing all types of spirochetes were used, or the highly prevalent periodontal pathogen Treponemas were analyzed, spirochetes were observed in the brain in more than 90% of AD cases.
- Borrelia burgdorferi (Lyme disease agent) was detected in the brain in 25.3% of AD cases analyzed and was 13 times more frequent in AD compared to controls.
- The pathological and biological hallmarks of AD were reproduced in vitro by exposure of mammalian cells to spirochetes.
 APOE gene variants: Genes are one of many risk factors for dementia.
APOE gene variants: Genes are one of many risk factors for dementia.
- 25% of Alzheimer’s patients have a strong family history of the disease, only 1% directly inherit a gene mutation that causes early-onset Alzheimer’s
- APOE can influence your risk for the more common late-onset type of Alzheimer’s.
- three types of the APOE gene, called alleles: APOE2, E3 and E4.
- Everyone has two copies of the gene and the combination determines your APOE “genotype”—E2/E2, E2/E3, E2/E4, E3/E3, E3/E4, or E4/E4.
- The E2 allele is the rarest form of APOE and carrying even one copy appears to reduce the risk of developing Alzheimer’s by up to 40%.
- APOE3 is the most common allele and doesn’t seem to influence risk.
- The APOE4 allele, present in approximately 10-15% of people, increases the risk for Alzheimer’s and lowers the age of onset.
- Having one copy of E4 (E3/E4) can increase your risk by 2 to 3 times while two copies (E4/E4) can increase the risk by 12 times [2].
- Despite this association, the National Institutes of Health only recommends genetic testing for APOE status to advance drug research in clinical trials.
- Approximately half the population with double APO E4 genotype have Alzheimer’s by 65
- nearly 100% by age 80
Reversal of cognitive decline: A novel therapeutic program
Dale E. Bredesen AGING, September 2014, Vol 6 N 9
- Abstract: This report describes a novel, comprehensive, and personalized therapeutic program that is based on the underlying pathogenesis of Alzheimer’s disease, and which involves multiple modalities designed to achieve metabolic enhancement for neurodegeneration (MEND)
- The first 10 patients who have utilized this program include patients with memory loss associated with Alzheimer’s disease (AD), amnestic mild cognitive impairment (aMCI), or subjective cognitive impairment (SCI).
- Nine of the 10 displayed subjective or objective improvement in cognition beginning within 3-6 months, with the one failure being a patient with very late stage AD.
Reversal of cognitive decline in Alzheimer’s disease.
Bredesen,et al Aging (Albany NY). 2016 Jun
- 66yo male with 2 years of memory impairment including difficulty at work.
- Positive amyloid PET and reduced hippocampal volume.
- Neuropsych testing=Dx with MCI (mild cognitive impairment) strong family history, APOE4.
- 10months of MEND protocol=from 17th to 70th percentile for hippocampal volume,
- Significant memory improvement in 3 months.
MEND (Metabolic Enhancement for NeuroDegeneration) protocol results
- Six of the patients had had to discontinue working or were struggling with their jobs at the time of presentation.
- All were able to return to work or continue working with improved performance.
- Improvements have been sustained, and at this time the longest patient follow-up is two and one-half years from initial treatment, with sustained and marked improvement.
Subtypes of Alzheimer’s disease based on the predominant driver
- Type 1-Inflammatory: triggered by infection, inflammation-inducing diet, leaky gut, chronic insulin resistance
- Type 2-Atrophic: triggered by shortage of nutrients, hormones, and trophic factors that support neuronal function
- Type 3-Toxic: triggered by exposure to toxic metals, xenobiotics, or mycotoxins.
Insulin resistance is intimately connected to AD. It drives systemic inflammation, and indirectly leads to amyloid plaque buildup.
 Therapeutic goals
Therapeutic goals
- Slows progressive damage-by reducing inflammation
- Improve cellular energy
- Increase blood flow to the brain
- Exercise and exercise the neurons(brain training)
- Provide and stimulate growth factors
- Remove Toxins and infections
- Identify and Modify risk factors including labs.