A PLANT-BASED DIET AND CORONARY ARTERY DISEASE: A MANDATE FOR EFFECTIVE THERAPY
Caldwell B Esselstyn MD, Journal of Geriatric Cardiology, May 2017; 14(5): 317–320. Cleveland Clinic, Center for Integrative & Lifestyle Medicine.
Background
A 1999 autopsy study of young adults in the US between the ages of 17 and 34 years of who died from accidents, suicides, and homicides confirmed that coronary artery disease (CAD) is ubiquitous in this age group. The disease process at this stage is too early to cause coronary events but heralds their onset in the decades to follow.[1] These data are similar to those reported in an earlier postmortem analysis of US combat casualties during the Korean conflict, which found early CAD in nearly 80% of soldiers at an average age of 20 years.[2] From these reports, which are 17 and 63 years old, respectively, it is clear that the foundation of CAD is established by the end of high school. Yet, medicine and public health leaders have not taken any steps to forestall or eliminate the early onset of this epidemic. Smoking cessation, a diet with lean meat and low-fat dairy, and exercise are generally advised, but cardiovascular disease (CVD) remains the number one killer of women and men in the US. The question is, why? Unfortunately, such dietary gestures do not treat the primary cause of CVD. The same can be said of commonly prescribed cardiovascular medications such as beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, anticoagulants, aspirin, and cholesterol lowering drugs and medical interventions such as bare metal stents, drug-eluting stents, and coronary artery bypass surgery.
It is increasingly a shameful national embarrassment for the United States to have constructed a billion-dollar cardiac healthcare industry surrounding an illness that does not even exist in more than half of the planet. If you, as a cardiologist or a cardiac surgeon, decided to hang your shingle in Okinawa,[3] the Papua Highlands of New Guinea,[4] rural China,[5] Central Africa,[6] or with the Tarahumara Indians of Northern Mexico,[7] you better plan on a different profession because these countries do not have cardiovascular disease. The common thread is that they all thrive on whole food, plant-based nutrition (WFPBN) with minimal intake of animal products.
By way of contrast, in the United States, we ignore CVD inception initiated by progressive endothelial injury, inflammatory oxidative stress, decreased nitric oxide production, foam cell formation, diminished endothelial progenitor cell production and development of plaque that may rupture and cause myocardial infarction or stroke.[8] This series of events is primarily set in motion, and worsened, by the Western diet, which consists of added oils, dairy, meat, fish, fowl, and sugary foods and drinks—all of which injure endothelial function after ingestion, making food a major, if not the major cause of CAD.[9]
In overlooking disease causation, we implement therapies that have high morbidity and mortality. The side effects of a plethora of cardiovascular drugs include the risk of diabetes, neuromuscular pain, brain fog, liver injury, chronic cough, fatigue, hemorrhage, and erectile dysfunction. Surgical interventions are fatal for tens of thousands of patients annually. Each year approximately 1.2 million stents are placed with a 1% mortality rate, causing 12,000 deaths, and 500,000 bypass surgeries are performed with a 3% mortality rate, resulting in another 15,000 deaths. In total, 27,000 patients die annually from these two procedures.[10] It is as though in ignoring this dairy, oil, and animal-based illness, we are wedded to providing futile attempts at temporary symptomatic relief with drugs and interventional therapy, which employs an unsuccessful mechanical approach to a biological illness with no hope for cure. Patients continue to consume the very foods that are destroying them. This disastrous illness and ineffective treatments need never happen if we follow the lessons of plant-based cultures where CVD is virtually nonexistent.
Treating the cause
In 1985, I initiated a small study utilizing WFPBN in 24 patients who were severely ill with CAD. The moment of truth came a year later for a patient in his 50 s with significant vascular disease in his heart and right leg. At study onset, while crossing a skyway into the Cleveland Clinic he experienced claudication that forced him to stop and rest five times. Results of a pulse volume study revealed a markedly diminished right ankle pulse. Following nine months of WFPBN, all claudication had resolved, and a repeat pulse volume was double that of his baseline.[11] As statin drugs were not yet available, this was proof of the concept that WFPBN alone can halt and reverse CVD.
After 12 years, we reviewed the CVD events of our 18 adherent patients. During the eight years prior to entering our study, while in the care of expert cardiologists, they had sustained 49 cardiac events, which was indicative of disease progression. In contrast, 17 of the 18 patients sustained no further events during the 12 years they spent in our study. One patient who was initially adherent developed angina and required bypass surgery six years after resuming a Western diet. These findings illustrate the need for close adherence with WFPBN.[12]
Twelve patients in our initial group had a follow-up angiogram. There was significant disease reversal in four of them, which suggests that WFPBN could not only eliminate future cardiac events but could also reverse angiographic disease. Even if significant angiographic reversal does not occur, patients can still benefit from more subtle improvements in the overall health of their endothelial cells and their capacity to produce nitric oxide, eliminating angina and future CVD events.[12] Additionally, the robust antioxidant value of WFPBN diminishes oxidative inflammation in plaques and foam cells, thus strengthening the cap over the plaques (Figure 1).
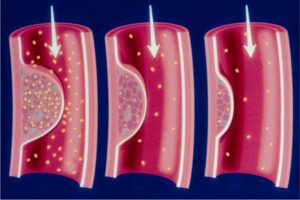
Progressive plaque cap thickening (white arrow) and plaque shrinkage accomplished with plant-based nutrition
A strengthened cap is unlikely to rupture, and adherent participants have been empowered to make themselves “heart attack proof” without the additional expense or risk of ineffective drugs, stents, or bypass surgery.
In 2014, we conducted a second larger study of 198 patients with significant CAD.[9] Of these patients, 119 had undergone a prior coronary intervention with stents or bypass surgery, and 44 had a previous heart attack. There were multiple comorbidities including hypercholesterolemia, hypertension, obesity, and diabetes. During four years of follow up, 99.4% of the participants who adhered to WFPBN avoided any major cardiac event including heart attack, stroke, and death, and angina improved or resolved in 93%. Of the 21 non-adherent participants, 13 (62%) experienced an adverse event. When comparing these results to the well-known COURAGE,[13] and Lyon Diet Heart Study,[14] which consisted of conventionally treated participants, there is beyond a 30-fold difference in major cardiovascular events favoring WFPBN.
In 1990, Ornish, et al.,[15],[16] utilized a low-fat vegetarian diet without added oil and stress management instruction to arrest CAD and reverse angiographic disease, which was confirmed in subsequent publications. Earlier, in 1951, Strom and Jensen reported a profound decrease in circulatory diseases in Norway during WWII when the Germans confiscated the country’s livestock, forcing the Norwegians to subsist mostly on plant food.[17] Results from both the On-Target Transcend trial investigators,[18] and the Epic Oxford Study[19] with more than 75,000 participants support the power of nutrition for primary and secondary CVD prevention.
In the early 1970s, Finland (and especially its eastern province of Karelia) was the heart disease capital of the world. Health authorities and local officials there became intent on educating the public on how to reduce cholesterol, blood pressure, and intake of animal foods and stop smoking. This group reduced their intake of dietary saturated fat, increased vegetable consumption, and decreased their smoking rate from 52% to 31%. During the next 30 years, Karelia’s CAD disease rate plummeted by 85%. For Finland as a whole, CAD decreased by 80%.[20]
Researchers at Cleveland Clinic under the direction of Stanley Hazen, which included Tang,[21] Koeth,[22] and Wang,[23] studied the metabolism of lecithin and carnitine found in eggs, meat, milk and diary products, liver, shellfish, and fish. The intestinal microbiota of omnivores metabolizes these substances producing trimethylamine oxide (TMAO), which causes vascular injury. This investigation was a powerful validation for WFPBN because ingestion of these animal foods by persons who strictly consume plants produces no TMAO. In fact, plant eaters do not have intestinal bacteria capable of producing TMAO.
The totality of converging lines of evidence, including epidemiology, wartime deprivation, large nutritional cohort population transitioning studies, and randomized and non-randomized investigations point to nutrition as the principle etiological factor in atherosclerotic CVD.
What is withholding the cure?
For years, I have resisted making the suggestion that compensation could be an issue in decision-making. However, multiple lawsuits have arisen in cases where unnecessary stenting or bypass surgery was performed for nonexistent or minimal lesions.[24],[25] Results of multiple investigations consisting of thousands of patients all show that stenting in an emergency situation is lifesaving while at the same time fails to prolong life or protect against future heart attacks in most patients undergoing elective stent placement when compared with optimal medical therapy. It is particularly disingenuous for physicians to tell patients that they are a walking time bomb—frightening them into accepting a procedure fraught with potential morbidity and possible mortality that is also non-curative—after an angiogram confirms a 90% blockage. Present day angiography does not identify, and angioplasty does not treat, the lesions that are most likely to cause a heart attack.[26]
Accepting the fact that most cardiovascular physicians are honest, caring, and compassionate, why do they resist WFPBN? Cardiovascular medicine practitioners receive essentially no nutrition education in medical school or postgraduate training. Therefore, they lack not only the skill set needed to help their patients modify their diets but also a basic awareness that plant-based nutrition can halt and reverse CVD. I recall a lawyer with CAD and angina who rapidly improved following WFPBN. He became quite angry after a follow-up visit to his cardiologist who said he knew WFPBN might be successful. The lawyer asked, “Why didn’t you offer it to me many months ago?” and the cardiologist replied, “In my experience patients won’t follow that program.” Where upon the lawyer stated, “That must be my decision, not yours.” It is not the message that is wrong but how and if the message is articulated that determines adherence and success.
Without a randomized controlled trial, can a physician feel secure recommending a plant-based option? Absolutely! Results from the COURAGE TRIAL[13] confirmed that stenting in stable patients was not superior to optimal medical therapy. The prompt, powerful, and enduring effects of WFPBN were recorded by Massera, et al.,[27] who reported dramatic reversal of crippling angina in a man who refused medication or surgical procedures but agreed to WFPBN. The man can now run four miles without symptoms.
In summary, current palliative cardiovascular medicine consisting of drugs, stents, and bypass surgery cannot cure or halt the vascular disease epidemic and is financially unsustainable. WFPB can restore the ability of endothelial cells to produce nitric oxide,[28] which can halt and reverse disease without morbidity, mortality, or added expense. As powerful as the data are, it is unconscionable not to inform the cardiovascular disease patient of this option for disease resolution. To begin to eliminate chronic illness, the public needs to be made aware that a pathway to this goal is through WFPBN.
References
- Strong JP, Malcom GT, McMahan C, et al. Prevalence and extent of atherosclerosis in adolescents and young adults: Implications for prevention from the pathobiological determinants of atherosclerosis in youth study. JAMA. 1999;281:727–735. [PubMed] [Google Scholar]
- Enos WF, Holmes RH, Beyer J. Coronary disease among united states soldiers killed in action in korea: Preliminary report. JAMA. 1953;152:1090–1093. [PubMed] [Google Scholar]
- Willcox BJ, Willcox DC, Todoriki H, et al. Caloric restriction, the traditional Okinawan diet, and healthy aging: the diet of the world’s longest-lived people and its potential impact on morbidity and life span. Ann N Y Acad Sci. 2007;1114:434–455. [PubMed] [Google Scholar]
- Sinnett PF, Whyte HM. Epidemiological studies in a total highland population, Tukisenta, New Guinea. Cardiovascular disease and relevant clinical, electrocardiographic, radiological and biochemical findings. J Chron Dis. 1973;26:265–290. [PubMed] [Google Scholar]
- Campbell TC, Parpia B, Chen J. Diet, lifestyle, and the etiology of coronary artery disease: the Cornell China study. Am J Cardiol. 1998;82:18T–21T. [PubMed] [Google Scholar]
- Miller K, Rubenstein A, Åstrand P. Lipid values in Kalahari Bushmen. Arch Intern Med. 1968;121:414–417. [PubMed] [Google Scholar]
- Connor WE, Cerqueira MT, Connor RW, et al. The plasma lipids, lipoproteins, and diet of the Tarahumara Indians of Mexico. Am J Clin Nutr. 1978;31:1131–1142. [PubMed] [Google Scholar]
- Nabel EG, Braunwald E. A tale of coronary artery disease and myocardial infarction. New Engl J Med. 2012;366:54–63. [PubMed] [Google Scholar]
- Esselstyn CB, Jr, Gendy G, Doyle J, et al. A way to reverse CAD? J Fam Pract. 2014;63:356–364. [PubMed] [Google Scholar]
- Peterson ED, Jollis JG, Bebchuk JD, et al. Changes in mortality after myocardial revascularization in the elderly: the national medicare experience. Ann Intern Med. 1994;121:919–927. [PubMed] [Google Scholar]
- Esselstyn CB., Jr Prevent and reverse heart disease. Prog Clin Biol Res. 2007:347–355. [Google Scholar]
- Esselstyn CB., Jr Updating a 12-year experience with arrest and reversal therapy for coronary heart disease (an overdue requiem for palliative cardiology) Am J Cardiol. 1999;84:339–341. [PubMed] [Google Scholar]
- Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. New Engl J Med. 2007;356:1503–1516. [PubMed] [Google Scholar]
- de Lorgeril M, Salen P, Martin JL, et al. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation. 1999;99:779–785. [PubMed] [Google Scholar]
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336:129–133. [PubMed] [Google Scholar]
- Ornish D. Avoiding revascularization with lifestyle changes: The Multicenter Lifestyle Demonstration Project. Am J Cardiol. 1998;82:72t–76t. [PubMed] [Google Scholar]
- Strom A, Jensen RA, Oslo MD, Oslo MD. Mortality from circulatory diseases in Norway 1940–1945. Lancet. 1951;257:126–129. [PubMed] [Google Scholar]
- Dehghan M, Mente A, Teo KK, et al. Relationship between healthy diet and risk of cardiovascular disease among patients on drug therapies for secondary prevention: a prospective cohort study of 31,546 high-risk individuals from 40 countries. Circulation. 2012;126:2705–2712. [PubMed] [Google Scholar]
- Crowe FL, Appleby PN, Travis RC, Key TJ. Risk of hospitalization or death from ischemic heart disease among British vegetarians and nonvegetarians: results from the EPIC-Oxford cohort study. Am J Clin Nutr. 2013;97:597–603. [PubMed] [Google Scholar]
- Puska P, Salonen J, Nissinen A, Tuomilehto J. The North Karelia project. Rev Epidemiol Sante Publique. 1983;12:191–195. [PubMed] [Google Scholar]
- Tang WHW, Wang Z, Levison BS, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. New Engl J Med. 2013;368:1575–1584. [PMC free article] [PubMed] [Google Scholar]
- Koeth RA, Wang Z, Levison BS, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19:576–585. [PMC free article] [PubMed] [Google Scholar]
- Wang Z, Klipfell E, Bennett BJ, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature. 2011;472:57–63. [PMC free article] [PubMed] [Google Scholar]
- Authorities: Doctor performed unecessary medical procedures as part of scheme. [accessed March 7, 2017]. http://fox8.com/2014/08/21/authorities-doctor-performed-unnecessary-medical-procedures-as-part-of-scheme/
- Stent scandal: a shocking story, but not news. [accessed March 7, 2017]. http://www.healthbeatblog.com/2010/12/stent-scandal-a-shocking-story-but-not-news/
- Forrester JS, Shah PK. Lipid lowering versus revascularization: an idea whose time (for testing) has come. Circulation. 1997;96:1360–1362. [PubMed] [Google Scholar]
- Massera D, Zaman T, Farren GE, Ostfeld RJ. A whole-food plant-based diet reversed angina without medications or procedures. Case Rep Cardiol. 2015;2015:978906. [PMC free article] [PubMed] [Google Scholar]
- Ornish D, Brown S, Scherwitz L, et al. Can lifestyle changes reverse coronary heart disease? Lancet. 1990;336:624–626. [PubMed] [Google Scholar]